Medically reviewed by Anne Peled, M.D. and Elisabeth Potter, M.D.
Every patient is unique, so how do you know which breast reconstruction is right for you?
The Breastie’s Guide to Reconstruction is meant to be an entry into the world of breast reconstruction. You will find a non-comprehensive overview of terms related to breast reconstruction, including reconstruction types, potential complications, and alternatives.
The purpose of this guide isn’t to say one reconstruction is better than another, but to give you the language you need to find out what works best for you.
Quick Links
- Choosing the Best Reconstruction for You
- Working With Your Plastic Surgeon
- Implant-Based Reconstruction
- Autologous Reconstruction
- Aesthetic Flat Closure
- Fat Grafting
- Nipple and Areola Reconstruction
- Nerve Preservation
Choosing the Best Reconstruction for You
Breast reconstruction is an incredibly personal choice and the ultimate goal should not be about aesthetics, but about how you feel in your body; being comfortable should always be your North Star. However, what that means is different for everyone.
To help you explore which type of reconstruction will help you feel the best in your body, The Peak has compiled a list of self-reflection questions. We invite you to use this as journal prompts or conversation starters ahead of your plastic surgery consultations so that you may go into those meetings feeling empowered and in charge.
Remember, every Breastie will have a different answer to these questions and even those with similar answers may find that different types of breast reconstruction suit their needs.
It is equally important to remember that your answer to these questions is a snapshot of your life at a specific moment in time. If you were to ask yourself these questions in a year from now or in ten years from now, you will likely have different answers.
The good news is that for most patients, it is never too late to change your mind: breast reconstruction does not have to be permanent. Someone who chooses implant-based reconstruction now may opt to go flat in the future and someone who chooses to go flat now can choose to reconstruct breasts with autologous reconstruction down the line.
Self-Reflection Questions
- How do you feel about your breasts? What do you like about them and what don’t you like about them?
- Where are you in your life right now? Do you live an active lifestyle or have other factors, such as young children or a particular line of work, that require you to be mobile?
- What types of activities do you engage in regularly? What role do your chest and abdominal muscles play in those activities?
- How much time are you willing to dedicate to your reconstruction right now? If oncologically safe, how quickly would you like to complete your breast reconstruction?
- How important is chest sensation to you? Is maintaining sensation to your chest something that is important to you?
- If it is oncologically safe, do you have a preference about the placement of your scars?
Working With Your Plastic Surgeon
Now that you know what your goals are for your reconstruction, it’s important to work with your plastic surgery team to realize those goals.
This is often referred to as shared-decision making: the act of working with your healthcare team to jointly make decisions about your care. This is key because while your healthcare providers have a wealth of knowledge in their areas of expertise, no one knows your body like you do.
Below are some questions you can bring to your consultation to make sure you are on the same page.
Questions to Ask Your Surgeon
- What types of breast reconstruction do you specialize in?
- What type of reconstruction would you recommend for me and why? What would the scar placement look like?
- What timelines can I expect for my reconstruction?
- How do you recommend I care for my scars following surgery?
- What type of follow-up care can I expect once my reconstruction is complete?
- Do you have before-and-after photos of the type of surgery you recommend for me?
- Can I talk to another patient who has been through or who is going through this experience?
- For those interested in autologous reconstruction:
- Will any of my muscles be cut or removed?
- Under what circumstances might you change from a technique that does not touch the muscle to one that impacts some or all of my muscles during the surgery? Can we create a plan in case that happens?
- If I were to change my mind in five, ten, or 20 years from now, will I be able to opt for a different type of reconstruction? What limitations might I have?
- If needed, can you refer me to someone who specializes in other types of reconstruction?
Implant Reconstruction
Implant-based reconstruction: Once the breast tissue is removed, implants are used either on their own or in conjunction with other tissue to rebuild a breast.
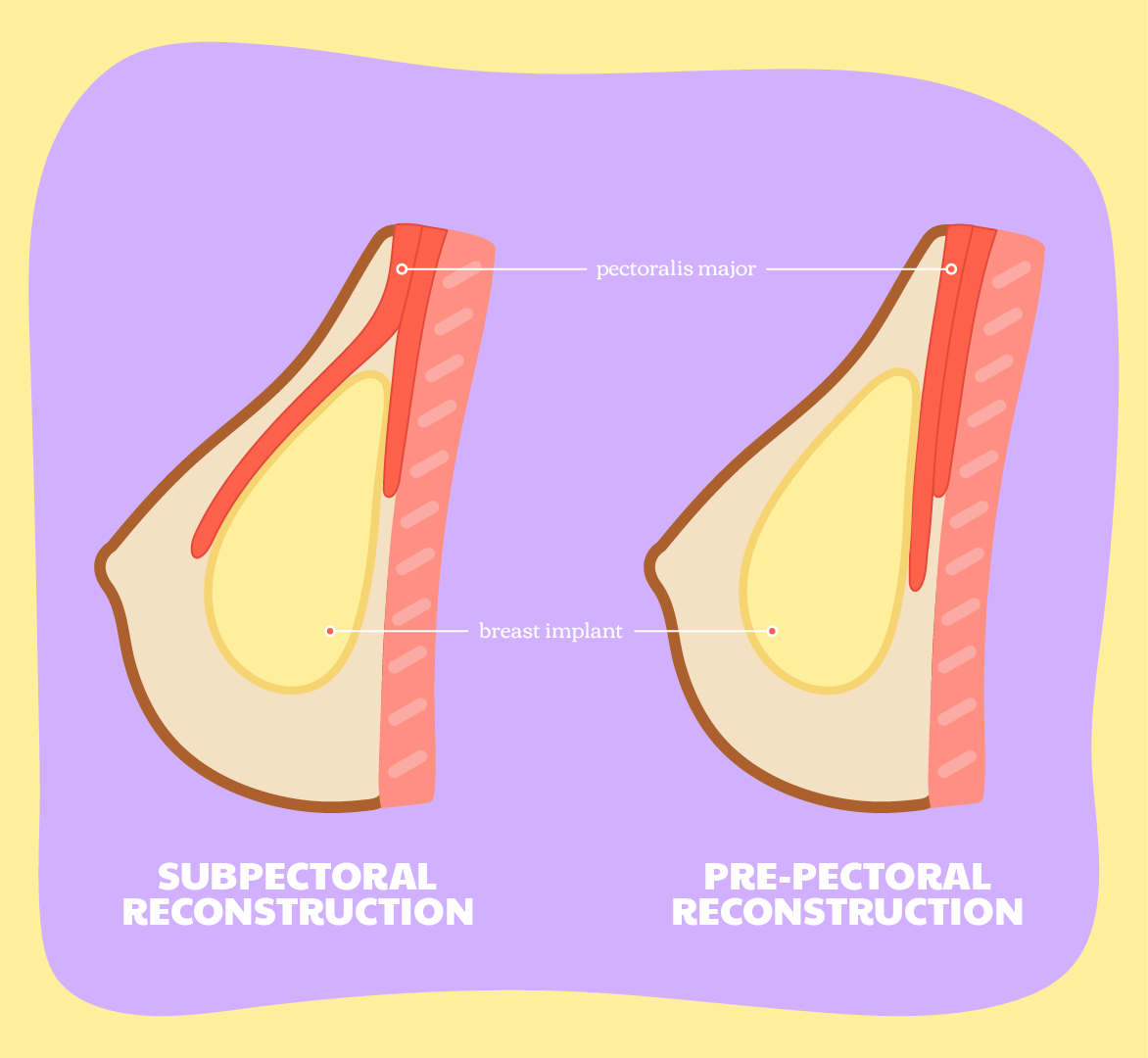
Over the muscle (OTM): In which implant(s) are placed on top of the pectoral muscle, also known as pre-pectoral reconstruction.
Under the muscle (UTM): In which implant(s) are placed below the pectoral muscle, also known as subpectoral reconstruction.
Breast tissue expanders: A thick-walled silicone balloon is implanted under the breast skin, tissue, and, in certain cases, muscle, to be filled with a saline solution progressively so as to stretch the tissue to make space for the implant size of choice. Those who require breast tissue expanders will require at least two surgeries to complete their breast reconstruction.
Implant types
Silicone-filled breast implants: A silicone outer shell, which can be smooth or textured, is filled with silicone gel.
Saline-filled breast implants: A silicone outer shell, which can be smooth or textured, is filled with saline (sterile salt water). Should the outer shell break, the saline solution can be absorbed by the body.
Structured saline implants: Implants filled with sterile salt water but, unlike their traditional saline counterparts, contain a structure to give the implant a natural shape.
Gummy bear implants: Form-stable implants filled with a silicone gel that is thicker in consistency than traditional silicone implants, meaning that they maintain their shape even if their textured outer shell is broken.
Round implants: Implants are round in shape.
Teardrop implants: Implants are similar in shape to a teardrop, with more volume at the bottom than at the top.
Smooth implants: A smooth outer shell coats these implants, meaning they move more freely within the implant pocket. Most round implants used have a smooth shell, as round implants do not need to adhere to the pocket in a certain orientation the way teardrop implants do.
Textured implants: Implants with a velcro-like outer shell, which allows implants to stick to the capsule over time, which is especially important for teardrop-shaped implants so that they may remain in the correct orientation.
There is a known link between textured implants and breast implant-associated anaplastic large cell lymphoma (BIA ALCL) and, as a result, certain textured breast implants have been restricted by health authorities (see: Breast Implant-Associated Anaplastic Large Cell Lymphoma).
Related Terms
Direct-to-Implant: A reconstruction that is completed at the same time as a mastectomy, in which implants are placed by a plastic surgeon immediately following the removal of the breast tissue.
Not all individuals may be a candidate for a direct-to-implant reconstruction and a direct-to-implant reconstruction does not guarantee that an individual will only require one surgery.
Staged Reconstruction: A reconstruction that is completed in multiple stages, with more than one surgery. In a typical staged reconstruction, a plastic surgeon will place tissue expanders following the removal of the breast tissue during the mastectomy during one procedure while the tissue expanders will be switched for implants or flaps in a later procedure, also referred to as an exchange surgery.
Breast Implant-Associated Anaplastic Large Cell Lymphoma (BIA ALCL): A rare type of non-Hodgkin's lymphoma that has been found in the capsule and fluid around certain breast implants. To date, all patients who have been diagnosed with BIA ALCL have a history of having had textured implants at some point in their implant journey.
When diagnosed early, the prognosis from BIA ALCL is very good, with treatment usually consisting of removal of the implants and implant capsules and possibly other treatment like chemotherapy.
In July 2019, the FDA issued a recall for specific models of Allergan textured breast implants due to the risk of BIA-ALCL. The agency continues to monitor instances of BIA ALCL.
Breast implant illness (BII): A term used to describe a range of symptoms that are reported to occur in some after undergoing breast reconstruction or cosmetic surgery involving breast implants.
Because it is not well understood, BII is not recognized as a medical condition, though many symptoms, such as brain fog, fatigue, joint and muscle pain, and weight changes, are associated with autoimmune and connective tissue disorders. Some who experience BII say symptoms improve upon the removal of their implants, but more research is needed to understand the link between implants and the reported symptoms.
Capsular Contracture: Once an implant is placed, a capsule of scar tissue forms around it as a natural part of the healing process. However in some cases, this capsule can become hard and tight, and potentially make the breast feel hard to the touch, cause pain, and impact the look of the breast by distorting the implant.
If capsular contracture happens, it can possibly be treated with non-invasive treatments such as medications or physical therapy, but sometimes requires further surgery to release or remove the capsule.
Autologous Reconstruction
Autologous tissue reconstruction: A procedure in which breasts are reconstructed using tissue from elsewhere on your body. The tissue typically includes fat, skin, and blood vessels, while certain procedures also use muscle (see: perforator flap).
Free flap: A procedure in which the tissue being used to rebuild breast mounds is entirely removed from the body before being reattached through microsurgery to reconnect the blood vessels that will supply the area with blood.
Pedicled flap: A procedure in which tissue from another area of the body is brought to the chest area to reconstruct breast mounds without being disconnected from its blood vessels, typically through tunnels under the skin. Also known as an attached flap procedure.
Perforator flap: A procedure in which tissue that does not include muscle is used to reconstruct breast mounds. Some autologous reconstructions may be referred to as muscle-sparing. These are different from perforator flaps as they still involve some of the muscle in the affected area.
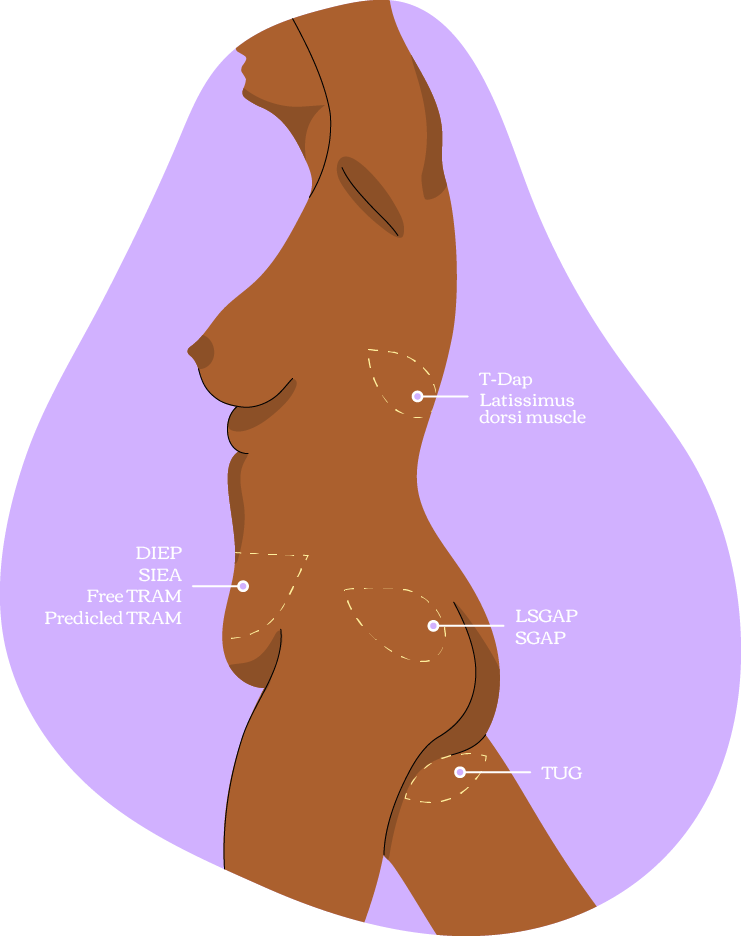
Latissimus dorsi flap: A pedicled (attached) procedure in which a flap including skin, fat, blood vessels, and the latissimus dorsi muscle, located in the upper back below the shoulder and behind the armpit, is used to recreate breasts.
Goldilocks: A technique in which some of the skin and the fat underneath the skin that was spared during the mastectomy is used to reconstruct breasts.
Microsurgical Techniques
Microsurgical reconstructive techniques require that very small blood vessels and/or nerves from the flap tissue be cut and then reattached to the chest. Because of the precision required for these surgeries, those who perform them must be trained in microsurgery.
Before undergoing a procedure that requires microsurgical techniques, a patient may have to undergo a scan so that the surgeon can verify that the blood vessels are suitable for the surgery.
TRAM flap: A procedure in which fat, skin, blood vessels, and part or the entirety of the transverse rectus abdominis muscle from the lower belly are used to reconstruct breasts. This reconstruction can be completed as a free flap, using microsurgery, or as a pedicled (attached) flap. Some TRAM flaps may also be muscle-sparing, meaning some but not all the muscle is impacted.
DIEP flap: A muscle-saving free flap procedure in which tissue, typically fat, skin, and blood vessels, are removed from the lower belly and used to reconstruct the breast. The blood vessels are connected to the chest using microsurgery.
DIEP flaps are similar to TRAM flaps, in that the tissue used is taken from the lower belly, but because the muscle is spared, they typically have a faster recovery time.
In early 2023, the procedure codes for certain autologous reconstruction, including the DIEP flap, had been eliminated, which limited access to the procedure. Thanks to patient advocacy, the codes were reinstated.
SIEA flap: A perforator free flap procedure in which fat, skin, and the superficial inferior epigastric artery blood vessel from the lower belly are used to recreate breasts.
Like the DIEP flap, microsurgery is used to reconnect the blood vessels to the chest. Unlike the similar DIEP flap, the SIEA flap leaves the fascia, which covers the rectus abdominis muscle, untouched.
However, many are not eligible for the procedure as the blood vessels may be too small or simply not exist, or they may have been previously cut during procedures such as a hysterectomy or c-section.
TUG flap: A procedure in which fat, skin, blood vessels, and part or the entirety of the transverse upper gracilis muscle from the upper inner thigh is used to reconstruct breasts using microsurgery.
PAP flap: A perforator free flap procedure in which the profunda artery perforator, a blood vessel that runs through the thigh, is used along with skin and fat from the back of the upper thigh below the buttock is used to recreate breasts. The blood vessels are reconnected to the chest using microsurgery.
Aesthetic Flat Closure
Aesthetic flat closure: Unlike other reconstructive techniques, the objective of aesthetic flat closure is not to rebuild breast mounds following a mastectomy, but to rebuild the shape of the chest wall to achieve a flat appearance.
While breast reconstruction is covered by the Women’s Health and Cancer Rights Act (WHCRA), there is no specific procedure code for aesthetic flat closure. As a result, surgeons are not able to easily bill – or be paid – for aesthetic flat closures and some insurance companies may refuse coverage.
Related Terms
Dog ears: An effect that can occur when tissue puckers at the end of a linear incision, causing the appearance of puffiness that resembles dog ears. These can be corrected with additional surgery.
Fat Grafting
Fat grafting: A procedure in which fat tissue is taken from another part of the body, such as the thighs or belly, processed, and then injected into the breast area to recreate breasts on its own or fill in specific areas as a complement to other techniques, such as implant-based or autologous reconstruction.
Nipple and Areola Reconstruction
Nipple and areola reconstruction: Nipple and areola reconstruction can be done following a non-nipple sparing mastectomy to give the appearance of nipples.
This can be achieved through surgery, using skin from the breast or a skin graft, to rebuild a nipple, or through a 3D tattoo that gives the appearance of an areola and nipple.
Nerve Preservation
Nerve preservation, or Resensation: Ideally done at the time of mastectomy, nerve preservation, or the preservation of sensation to the breast, can occur when the breast and plastic surgeons take care to keep as many nerves in the breast as intact as possible or reconstruct those that can’t be preserved.
By avoiding unnecessary harm to the nerves, a plastic surgeon who is specialized in microsurgical techniques may reconnect the cut nerves, either on their own or using a graft, to preserve sensation in the breast.
You can use Resensation’s Find a Surgeon tool to locate a provider in your area who uses nerve preservation techniques.
Related Reads
Top Questions to Ask Your Plastic Surgeon (According to an Expert)
Meet the Surgeon Who’s Combating Post-Mastectomy Pain Syndrome
Meet the Plastic Surgeon Pushing for Her Patients’ Say in Their Reconstruction